This page provides information about various conditions affecting the nose and sinuses.
Nasal Anatomy & Function
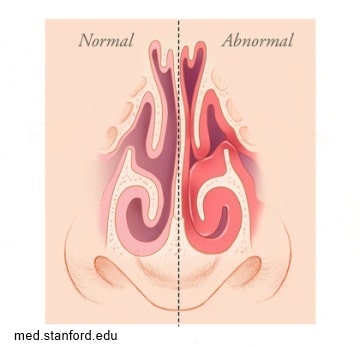
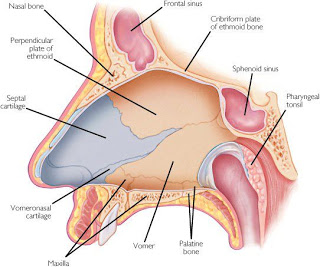
The inside of the nose is a complex area with intricate anatomy (structure) and physiology (function). Our nose is important for breathing, smell and taste, and sinus function. One important part is the nasal septum which is the wall separating the two nostrils and nasal passages. The septum is made up of cartilage and bone covered by mucosa. This thin wall made of cartilage is ideally located almost equally between your two nostrils which results in symmetric size of the nasal passages. However, some people have a deviated septum that they were either born with or developed somewhere along the way. It’s not necessary to have a perfectly straight septum; very few people do. A slightly off-center septum may not cause any problems, but a significantly deviated septum often causes noticeable symptoms and can be corrected through a procedure known as nasal septoplasty. In some cases a person with a mildly deviated septum has symptoms only when they have a cold or upper respiratory infection. In these patients the infection triggers increased nasal inflammation that temporarily amplifies any mild airflow problems related to the deviated septum. Once the cold resolves and the inflammation subsides, the symptoms usually resolve too.
A significantly deviated septum may cause:
- Blockage of one or both nostrils
- Chronic nasal stuffiness, one or both sides
- Recurrent sinus infections
- Postnasal drip
- Loud breathing
- Snoring
- Nosebleeds
- Sometimes headaches and facial pain
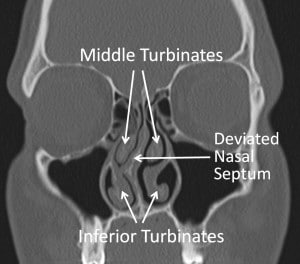
If these symptoms occur, surgery to correct the anatomic problem may be beneficial. Your physician may find that symptoms are stemming not only from a deviated septum, but also from swollen turbinates along the walls of your nasal passage.
Turbinates are shelves of bone that are covered with special mucosa. The mucosa can swell several times normal size. This can cause air flow to be blocked leading to the symptoms described above.
Septal abnormalities are not the only causes of nasal obstruction. Most people have intermittent obstruction on one side due to a normal process call the Nasal Cycle. This is a normal process in which the mucosa, or lining, on one side of the nose swells for several hours then switches to the other side, causing alternating nasal obstruction. Other causes result from mucosal inflammation. The mucosa is the lining of the nose; it is moist tissue like the lining of your mouth. When there is generalized mucosal edema (swelling) patients can have marked difficulty breathing through their nose. This can result from viral illness such as an upper respiratory infection, allergic rhinitis (seasonal allergies), cigarette smoke, or other causes of inflammation.
Septoplasty and Turbinoplasty
Septoplasty is a surgical procedure to correct a crooked septum that is causing symptoms with the goal of improving airflow and symptoms resulting from a deviated septum. The surgery is typically performed inside the nose by making small incisions in the mucosa and separating the mucosa from the underlying cartilage and bone. The crooked portions are then straightened or removed.
Turbinoplasty is a surgical procedure to reduce the size of the turbinates with the goal of improving airflow. The surgery is also done inside the nose. Generally the bone shelf is fracture outwards increasing the space, and the mucosa is treated to shrink it and prevent it from being able to expand.
It is routine for surgeons to perform both septoplasty and turbinate reduction surgery at the same time to completely eliminate associated symptoms. Since both procedures are relatively noninvasive, you will find that the recovery time is limited. The nose is a small area and after surgery there will be swelling caused by the surgery. This swelling can take several weeks to completely resolve. Most patients get considerable relief from previous symptoms and get back to life as normal within 1-2 weeks.
Risks of Surgery: Risks are uncommon, but can include the following
- Anesthesia risks. These are related to the process of general anesthesia are extremely rare. If you have a personal or family history of anesthesia related problems or a history of bleeding problems let your physician know.
- Bleeding. This can occur during or after the procedure. Some mild oozing is typical after surgery for a few days but major bleeding may require more treatment.
- Wound problems. These can include scaring, infection, abnormal healing, development of a hematoma (collection of blood in the surgical site) or abscess (infected fluid collecting in the surgical site).
- Residual disease or recurrent problems or dissatisfaction. Occasionally problems that we are trying to resolve or improve with surgery persist.
- Numbness or tenderness of the nasal tip. Sometimes the need to suture the septum causes mild irritation and sensitivity of the tip of the nose.
- Crusting. During the healing process crusting can develop it is usually temporary.
- Septal perforation. This occurs when a hole develops through the septum, it can be mild and undetectable or may lead to crusting, whistling, and irritation.
- Loss of smell. Very rare
- CSF leak. This is an extremely rare complication but more serious. CSF fluid surrounds the brain and can leak through fractures that could possibly occur during surgery.
- Change in nasal appearance. This is a very unlikely complication that can occur if too much cartilage is taken and nasal support is change the appearance may be affected.
Discharge instructions after septoplasty/turbinoplasty
- DIET- Generally, there are no food restrictions after surgery, but some physicians will recommend a soft diet during the recovery period. Starting immediately after surgery, patients may have fluids such as water or apple juice. Some patients experience nausea and vomiting after the surgery. This usually occurs within the first 24 hours and resolves on its own after the effects of anesthesia wear off. It is important to drink and remain hydrated for the first several days. Signs of dehydration include thick secretions, dark or infrequent urination, headache, or feeling unwell.
- PAIN –Pain is common but is usually mild. For mild to moderate pain Tylenol or Motrin are effective. For more severe pain a narcotic may be necessary.
- BLEEDING –After septoplasty it is normal to experience mild bleeding and oozing from the nose for the first 12-24 hours after surgery. You can remove the drip pad placed below your nostrils once the oozing has stopped. Keeping your head elevated at night or while sleeping will help to reduce this oozing. You should also avoid hot liquids and foods as they tend to dilate the blood vessels in your nose and increase oozing. Call your surgeon if your oozing requires more than 10 pads in 24 hours or if you experience brisk bleeding at any time.
- WOUND CARE –During the week after your septoplasty you will need to keep your nasal passages clean. You may have splints on either side of the septum. These splints vary, some have a small opening that will allow for easier breathing while in place and some are large porous sponges. A type of saline nasal spray will be recommended and can be used as often as once per hour to clean and flush out your nose after surgery even if splits are present. Continue to use nasal saline irrigation, for several weeks after surgery until the normal mucus production of your nose returns. It is optional but OK to gently clean your nostrils daily with water or half-strength peroxide or apply an antibiotic ointment inside each nostril.
- FEVER –Fever is not common but occasionally occur between 99 and 1O1 degrees for the first few days following surgery. Fever is worsened by a poor fluid intake producing dehydration. Fevers also can be reduced by encouraging being more active and taking deep breaths. Taking walks, deep sigh breaths, etc. may help.
- ACTIVITY –It is advisable to rest at home for the first 24 hours. During this time patients should be up and walking. The more you move around, the sooner you will start to feel better. Activity may be increased slowly, with a return to work after normal eating and drinking resumes, and pain medication is no longer required. Vigorous physical activity should be avoided for 14 days following surgery. Tobaccos use is prohibited after surgery, nicotine decreases blood flow to healing tissues and can compromise wound healing. There are no shower restrictions after surgery.
- FOLLOW UP –Please schedule a follow-up visit in 7 to 10 days as directed by your surgeon. During this visit, your surgeon will remove your nasal splints and clean the nasal cavities of any remaining debris. This can be mildly uncomfortable and it is a good idea to take either Tylenol or your prescribed pain medication just prior to this visit. Make sure that you have had something to eat prior to your appointment and consider having a companion available to drive you home after your appointment.
- MEDICATIONS –If you were using a topical nasal steroid spray prior to surgery, you can generally restart it after 72 hours or after your nasal splints have been removed. Be sure use your nasal steroid spray after using any nasal saline so that it is not washed out of the nose and be careful not to insert the tip of the spray bottle deeply into the nose.
Contact your physician if you have elevated fever, bleeding, dehydration, intractable pain, evidence of infection, purulent drainage from nose, or other concerns.